Government Tries to Reimbursement of Medicare Advantage. Will It Work? – Center for Retirement Research

Keeping health care costs under control is important for retirees.
Something good has happened lately. The Centers for Medicare and Medicaid Services (CMS) announced that its projected 2027 average increase in the rates Medicare pays for Medicare Advantage plans is expected to be only 0.09 percent. Analysts have predicted that 2027 rate increases will be 4 to 6 percent, in line with the 5.06 percent increase insurers are enjoying in 2026.
This proposal is a big deal because Medicare Advantage plans are a big deal. By 2025, most Medicare participants receive their benefits through a privately-insured Medicare Advantage plan instead of traditional government-run Medicare, a share that is expected to continue to rise over time (see Figure 1).
People gravitate toward Medicare Advantage plans for three reasons: 1) improved benefits, such as dental, vision, hearing, and fitness; 2) annual out-of-pocket cost limits for Part A and B services (unlike traditional Medicare); and 3) low or zero premiums. In return, enrollees must accept program procedures, such as pre-authorization to access care, and limited networks of health care providers. On balance, though, it’s clear why seniors tend to choose Medicare Advantage plans.
The biggest problem, however, is that Medicare Advantage plans are more expensive for Medicare. Congress’s Medicare Payment Advisory Commission estimated that payments for Advantage beneficiaries by 2025 were 20 percent higher than for traditional care. While Medicare usually pays for the services participants actually receive, the Medicare Advantage plan pays a fixed price per enrollment. That number is tied to local benchmarks, higher for higher-rated plans, and risk-adjusted to reflect the health status of each plan’s enrollees.
Because Medicare Advantage plans receive higher premiums for less healthy enrollees, insurers have an incentive to identify as many health conditions as possible for each enrollee. Not surprisingly, Medicare Advantage plans record more health conditions than traditional Medicare for comparable beneficiaries.
Analysts say the pattern is, at least in part, related to “chart reviews,” which insurers use to determine whether a person’s medical records match the information submitted by a provider. Although a chart review may identify an additional factor that may be contributing to a person’s health status, it may also identify diseases that are inaccurate, redundant, or unrelated to clinical care and therefore not relevant for billing purposes. By 2022, 62 percent of MA enrollees had a chart update, and these updates were more likely to add a diagnosis than subtract one.
CMS’s announcement to hold ongoing payments through 2027 for Medicare Advantage plans reflects the agency’s plan to update its risk adjustment model to better reflect current costs. A key part of that effort includes excluding statistical diagnostic information from chart reviews that may not be associated with a particular set of beneficiaries.
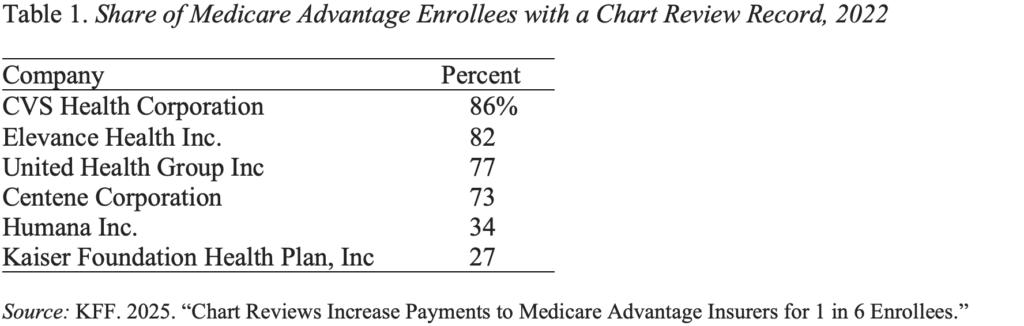
CMS will accept comments on the proposed fee increase until February 25, 2026, before publishing its final estimate on or before April 6, 2026. Obviously, this decision will have a major impact on companies that rely heavily on chart reviews (see Table 1).
CMS took a bold step; let’s hope the agency will continue with it. Keeping health care costs under control is critical to the financial security of current and future retirees.



